
Establishing New Treatment Directions For “Hard-To-Treat” Speech Sounds
Posted in: Communication Sciences Disorders
While most children outgrow common speech sound disorders — such as producing a “w” for an “r” — others persist in making speech sound errors, which can create academic and social issues that can persist for years.
Researchers Elaine Hitchcock of Montclair State University, Tara McAllister of New York University, and Jonathan Preston of Syracuse University, are working to change that.
Many people are aware that children with speech sound disorder exhibit atypical speech patterns that can result in reduced intelligibility. Speech intelligibility reflects how easily a child can be understood and poor speech intelligibility can pose a barrier to social and academic participation with potentially lifelong consequences for educational and occupational outcomes. Typically, delayed speech development resolves by 8-9 years old, but between 2-5% of children exhibit residual speech sound disorder (RSSD) which persists through adolescence. Children with RSSD commonly exhibit differences in phonological awareness, reading, and spelling. Differences in auditory perception of speech are also known to play a critical role in the development of typical speech production as well as literacy. This suggests that interventions enhancing auditory perception and providing feedback on the acoustics of speech errors could improve treatment outcomes for RSSD.
Consider Amanda Gorman, the Poet Laureate who spoke at the 2021 presidential inauguration. She clearly exemplifies a person with much to say, but who might not have always been understood. She describes having difficulty saying certain sounds, including “r” which she worked extremely hard to overcome with determination and hard work. But what if there were intervention techniques that decreased the challenge of acquiring difficult sounds such as “r”?
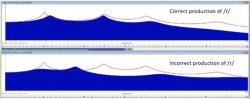
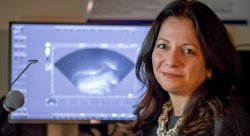
According to Hitchcock, McAllister and Preston, the use of acoustic and ultrasound biofeedback can significantly increase the accuracy of “r” pronunciation in children and adolescents, although few clinicians currently have access to this method as a means of speech sound intervention. Visual-acoustic biofeedback uses instrumentation to provide a real-time display of acoustic events such as formant patterns (Figure 1) and has been linked to positive outcomes in individuals with RSE who have not responded to previous intervention. Ultrasound biofeedback uses an ultrasound probe (Figure 2) – similar to ones used in cardiac and tissue imaging – which is held under the chin, and sound waves capture real-time images of the tongue. The images provide both the child and speech pathologist with information about the tongue’s position and shape.

Research suggests that visual biofeedback enhances the sensory experience of producing a sound like “r”. In addition to hearing the sound of speech, the child sees a visual display of her own speech and a model representing the correct pronunciation of the sound. The model creates a target. Using the visual display, the child can adjust her speech to achieve a better match with the target.
After a decade of testing these approaches with small scale studies, the research team has sufficient evidence to attribute the success of the treatment model to the unconventional approach it brings to the task of learning speech. In traditional methods, the clinician typically asks the child to imitate the “r” sound that they hear. However, many children who are unable to produce a clear “r” sound also have trouble hearing the difference between a clearly produced “r” and incorrect “r”. The theory is that biofeedback is successful because it bypasses that auditory channel. Even if the child can’t hear the difference between good and bad “r”, they can see whether they are matching the target on the screen. Matching the target lets them know if they are saying the “r” sound clearly.
Until recently, the research team was only able to offer these treatments via in-person services at Montclair, New York University or Syracuse University. Telepractice delivery of speech services has been increasing in recent years, with an explosive rise in the past two years due to the COVID-19 pandemic. Even after the pandemic subsides, a long-term shift toward greater use of telepractice is likely. Telepractice can improve flexibility for clients and clinicians and may be the only means for individuals in rural or underserved areas to access the services of a certified speech-language pathologist. Eliminating geographic barriers may also improve delivery of specialized services, such as visual biofeedback. Starting in February, 2022, both in-person and online treatment options using visual biofeedback are available for children ages 9-16.
Funded by the National Institutes of Health for in-person and online intervention options, the current research projects will meet a public health need by conducting the first randomized controlled trials comparing the efficacy and efficiency of speech intervention with and without real-time visual biofeedback. If you are interested in learning more about these research opportunities, please contact Elaine R. Hitchcock, PhD at MSUspeechstudy@gmail.com, Tara McAllister, PhD at NYUchildspeech@gmail.com, or Jonathan Preston, PhD at SpeechProductionLab@syr.edu.